


About skin cancer
Australia has one of the highest incidences of skin cancer in the world. The three major types of skin cancer are basal cell carcinoma (BCC), squamous cell carcinoma (SCC) and melanoma. SCCs and BCCs are the most common malignancies affecting humans.
The main risk factors for skin cancer are:
- Sun exposure, especially repeated severe sunburn. Up to 99% of all skin cancers are the result of sun exposure [1]. Exposure to UV radiation also includes use of solariums and tanning beds. Early life sun and UV exposure is particularly important, with excessive sun exposure during childhood and adolescence recognised to increase the risk of developing melanoma and non-melanoma skin cancers [2, 3].
- Increasing age
- Light skin that burns rather than tans and is freckly
- Previous skin cancer
- Family history of melanoma
- Multiple moles
- Rare pigment disorders, eg. xeroderma pigmentosum
Table of contents
Pre-Cancer
Pre-cancer is a term used to describe lesions on the skin that are not yet malignant, but have a very high risk of becoming malignant.
Solar (actinic) Keratosis
Solar keratoses are precursor lesions to SCCs. However, solar keratoses have a low risk of progression to SCC, and many regress spontaneously [4]. Solar keratoses are often multiple, flat lesions. Their surface is scaly or flaky and they are commonly red or skin-coloured lesions.

Bowen’s Disease
Bowen’s disease describes SCC localised to the epidermis (carcinoma in situ). Risk factors for the development of Bowen disease include:
- Sun (UV) exposure
- Arsenic exposure
- Exposure to ionising radiation
- Infection with the human papilloma virus when Bowen’s disease occurs on mucous membranes

Bowen’s disease is most commonly seen in older adults over 60 years of age. It affects both men and women and although it is more commonly seen on sun exposed areas, it can affect the skin on any part of the body [5].
Bowen’s disease typically appears as a well-demarcated plaque on the skin that grows slowly. It is pink-red in colour with a scaly surface and irregular edges [5]. There may be one solitary lesion, or several lesions. The lesions tend to be a few centimetres in size.
The biggest concern with Bowen’s disease is that the lesions may develop into invasive SCC, hence, lesions need to be treated.
Dysplastic Melanocytic Naevi
Dysplastic melanocytic naevi are lesions which are also referred to as atypical moles. They can occur on any part of the body, but are most commonly found on areas that are exposed to the sun. Dysplastic naevi tend to be larger than common moles, have irregular borders which may blend with the surrounding skin, have an uneven surface and often have several different colours. It is possible for dysplastic naevi to become a melanoma, however, most stay stable over time and do not become malignant. Dysplastic naevi need to be monitored for any changes, including size, shape and colour and should be protected from the sun [6].


Skin Cancer
Squamous Cell Carcinoma
Most SCCs are thought to arise from the aforementioned precursor lesions- solar keratoses and Bowen disease. SCCs have a variable spectrum; from localised, minimally invasive and easily managed lesions to invasive tumours which can spread to other organs and sites within the body [7]. Fortunately, most SCCs fall into the former category and are minimally invasive and easily controlled. Only a minority have the capacity to invade surrounding and distant tissues. SCCs that are more likely to invade tend to arise in areas that have previously been injured, such as over previous ulcers or scars, or those arising on mucous membranes, such as the lips [8].
SCCs arise from keratinising epithelial cells. They often appear like an ulcer on the skin or an erosion, but may also take on a blister-like appearance. They commonly have poorly-defined margins and can be fixed to surrounding structures [9].








Basal Cell Carcinoma
Basal cell carcinomas are the most common form of skin cancers. These arise from the basal cells which lie deep in the epidermis. They are commonly found on areas of the skin which receive the greatest amount of sun exposure – the head, neck, arms and legs. BCCs occur predominantly in the over 50 age group. It is estimated that BCCs account for ¾ of all non-melanoma skin cancers [10]. BCCs often present as lesions that do not heal – patients often describe a lesion that initially bled, then healed after a period of time, only to grow back again. The edge of a BCC is often rolled and the lesion itself often looks like an ulcer. BCCs are translucent and often have a network of ‘spider veins’ known as telangiectasia [10]. They rarely exhibit metastatic behaviour. Those that do metastasise have generally been left neglected for a number of years, or the patient is receiving immunosuppressive therapy, or the tumour has recurred [11].
Basal cell carcinomas are subdivided into 4 broad categories:
Superficial BCC


Superficial BCCs are typically scaly, red plaques that may itch or bleed. They look similar to psoriasis or eczema. The borders of the lesion can be either irregular or regular. These tumours are typically slow growing and can be treated with topical chemotherapy agents. If topical chemotherapy is not tolerated, the lesions can be excised.
Nodular/ulcerative BCC
Nodular/ulcerative BCCs tend to be well-defined lesions that are typically painless. The edges appear waxy and have an ingrowth of blood vessels. These lesions are not aggressive; but recurrent lesions are larger and exhibit more aggressive characteristics. Excision is the preferred method of treatment, as recurrences are more common following curettage and electrodessication.

Sclerosing BCC
Sclerosing BCCs are hardened, plaque lesions that are commonly white-yellow in colour. They have ill-defined margins and can ulcerate over time. The tumours are aggressive and are often quite large. Mohs surgery is the recommended treatment for this type of BCC to ensure that the margins are clear.


Basisquamous BCC
These tumours are locally aggressive tumours which may metastasise (the risk of metastasis is increased if the tumour is recurrent or large in size). They can be confused clinically for squamous cell carcinoma or nodular BCC.
Melanoma
Melanoma is the most aggressive type of skin cancer and carries the worst prognosis. Melanoma tends to be diagnosed at an earlier age than the majority of other cancers. The mean diagnosis of melanoma occurs at 52; approximately 10-15 years earlier than other common cancers, such as prostate, lung, colon and breast cancer [12]. As with other skin cancers, sun exposure is a major risk factor in the development, however, evidence suggests that intermittent sun exposure is more important in the development of melanoma than a history of continuous sun exposure. It is hypothesised that one instance of blistering sunburn during childhood doubles one’s lifetime risk of developing melanoma [12]. Genetic factors have also been implicated in the development of melanoma, with around 15% of patients with melanoma reporting a family history of melanoma or dysplastic naevi [13].
Melanoma is a cancer which arises from melanocytes in the skin. Melanocytes are the cells which provide the skin with its colour and pigment.
There are 4 subtypes of melanoma:
Nodular Melanoma
Nodular melanomas are the most aggressive form of melanoma and have the worst prognosis. From the early stages, nodular melanomas grow downward through the epidermis to the underlying dermis. Once in the dermis, the nodular melanoma can spread to other parts of the body. This occurs primarily via the lymphatic system and to a lesser extent via the bloodstream. Nodular melanomas are so named because they often contain several nodules.


Superficial Spreading Melanoma
This is the most common form of melanoma. Superficial spreading melanomas spread in a horizontal fashion to the surrounding areas of the epidermis and in some cases to the superficial part of the underlying dermis. Exhibiting this pattern of growth, the melanoma is far less likely to enter the deep part of the dermis and hence it is difficult for tumour cells to enter the lymphatic and blood vessels and spread to other parts of the body. However, if left untreated, superficial spreading melanoma can adopt a vertical growth pattern and invade the deep part of the dermis, where it can spread to other parts of the body.


Acral lentiginous melanoma
This is a type of melanoma primarily affecting the palms of the hands and the soles of the feet. It is a moderately aggressive tumour. It initially exhibits a phase of horizontal growth where it spreads to surrounding areas of the epidermis. This phase is often short-lived and the tumours enter a vertical growth phase quite rapidly. Hence, these tumours are more aggressive than superficial spreading melanomas, but less aggressive than nodular melanomas.


Lentigo Maligna Melanoma
This is the least aggressive form of melanoma. Lentigo maligna melanomas have an extended horizontal growth phase and are least likely to adopt a vertical growth pattern and metastasise to distant sites. These are mainly found in the elderly in sun-exposed areas after a long period of sun exposure through outdoor occupations.


Superficial spreading, lentigo maligna and acral lentiginous melanoma have features which follow the ABCD rule:
Asymmetry: One half of the lesion has a different appearance to the other half
Border irregularity: the border of the lesion is often jagged and irregular
Colour: there is an uneven pigmentation to the lesion; may be several colours appearing on the surface of the lesion
Diameter: These melanomas are often more than 6mm in diameter

Nodular melanomas are different; they tend to exhibit symmetry and tend to be uniform in their pigmentation [14]
Treatment
Electrodessication and Curettage
Electrodessication and curettage is a popular technique utilised in the removal of premalignant lesions, SCC and BCCs. Electrodessication uses a high-voltage, low amperage current to destroy the tissue of the skin. The procedure for electrodessication and curettage is as follows:
- Estimated tumour margins are marked and a local anaesthetic is applied to the area
- Tumour is curetted until the lesion is removed
- An electrode is applied to the dermis underlying the excised lesion
- The electrode is applied until the dermis has a charred appearance
- The charred dermis is then removed by a curette
- The electrode is re-applied
- The procedures of curettage and electrodessication are repeated roughly 2-3 times [15]
Electrodessication and curettage produces best results when performed on regions which have a thick dermis layer, such as the back, arms and legs. In general, the wound heals rapidly and the rates of cure are high; however, this depends on the expertise and experience of the practitioner performing the procedure [15].
Potential complications associated with the procedure include:
- Keloids
- Hypertrophic scars
- Depressed scars
- Hypopigmentation
- Tissue contracture
This type of treatment is appropriate for tumours which measure less than 2cm on the extremities. Surgical excision is preferred; however, for recurrent lesions, aggressive tumours and tumours arising near old scars or in high-risk locations (eg. mucous membranes) [15].
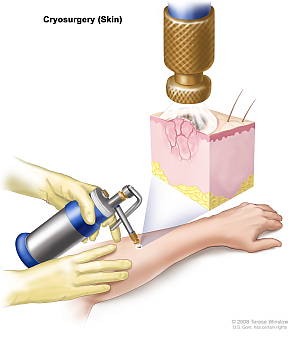
Cryosurgery
Cryosurgery involves ‘freezing’ off skin lesions using a gas. Liquid nitrogen is the most commonly used gas because it reaches a very cold temperature and is versatile. Cryosurgery can be used for pre-malignant lesions and for SCC and BCC. It also can be used for a range of other benign skin lesions. It is not indicated in the case of malignant melanoma [16]. Cryosurgery kills the cancerous cells in two main ways. Firstly, application of liquid nitrogen to the area causes ice crystals to form within the cells, which causes clotting during freezing. Secondly, when the tissue starts to thaw, blood flow to the area becomes stagnant, leading to ischaemic necrosis (tissue death) in the area [15]. Local anaesthesia may or may not be required during cryosurgery; this depends on the preference of the patient and the site of treatment [17].
There are several different cryotherapy techniques. These are outlined in table 1.
Cryptherapy Techniques
| Technique | Explanation |
| Dipstick Method | A cotton-tipped applicator is dipped into liquid nitrogen or another suitable gas and is applied to the treatment site/lesion. This process is repeated until the desired amount of freezing is achieved. Used for non-malignant lesions (lentigo, solar keratoses) |
| Open Spray | Liquid nitrogen is dispensed from a cryogun in spray form. The spray is dispensed 1-2cm from the lesion at a 90 degree angle in an intermittent fashion. Used for both benign and malignant lesions. Useful for curved surfaces and irregularly shaped lesions |
| Cryoprobe | This is also called contact therapy. It involves the application of a metal probe pre-cooled with a cryogen (e.g. liquid nitrogen) directly to the skin. Good for round lesions on flat surfaces. Primarily used in the management of benign skin lesions |
Table 1: Description of several cryotherapy techniques [16].

There are some groups of patients for whom cryosurgery is not indicated. There are some body sites that are not ideal locations for the application of cryosurgery, which include at the corners of the mouth, the border between the lips and the skin, skin overlying nerves, within the ear canal, the end of the nose and skin surrounding the eyes [16]. Cryosurgery is not indicated for patients with aggressive lesions, lesions with ill-defined margins and lesions that extend deep into the skin [15].

There are many advantages of cryosurgery, which include the following:
- Cost-effective
- Anaesthesia is not necessary; although patients can opt for local anaesthesia if desired
- Can be performed within the practice office
- Safe, simple
- No functional restrictions following the procedure
- Safe in pregnancy
- Produces a good 5 year cure rate in appropriately selected patients [16, 17]
However, there are some disadvantages associated with cryosurgery. Following the procedure, it is common for patients to experience tenderness, pain, swelling and redness. Other complications of the procedure include pigmentation changes, blister formation, infection, and damage to underlying structures, such as nerves and cartilage. Patients have reported lower rates of cosmetic and aesthetic satisfaction following cryosurgery compared to surgery and it can take a long time for cryosurgery wounds to heal [15].
Topical Agents
There are a number of topical chemotherapy agents that are used in the treatment of skin cancers.
5-fluorouracil was one of the first topical chemotherapy agents to be used for skin cancer. It is an anti-metabolite drug that decreases DNA synthesis and cell proliferation and growth, inducing cancer cell death. These effects are most marked in rapidly dividing cells, such as cancer cells [18]. 5-fluorouracil is safe and has a short treatment course, and is particularly effective in the treatment of solar keratoses. It is also used in the treatment of Bowen’s disease and actinic chelitis [15]. As with all treatments, there are several side effects associated with the use of topical 5-fluorouracil. Some of the commonly observed side effects include irritation, erythema, burning, pain and itch. There may also be changes in the pigmentation of the skin, crusting, swelling and oozing at the site [15].
Diclofenac is also used for topical treatment of skin cancer. Diclofenac is a non-steroidal anti-inflammatory drug which is primarily a cyclooxygenase-2 inhibitor. Diclofenac dampens the inflammatory response by reducing the synthesis of prostaglandins. The theory behind the use of diclofenac in the treatment of malignancies is that the production of prostaglandins from arachidonic acid helps to drive the induction of blood vessels into a tumour (angiogenesis), inhibits cell death (apoptosis), and increases the invasiveness of the tumour [18]. The main side effects of diclofenac topical treatment are local site reactions, such as itch, redness and dry skin. Less common adverse reactions include photosensitivity photocontact dermatitis. Diclofenac is used primarily for the treatment of solar keratoses [18].
Imiquimod is a drug that modifies the immune response. It is primarily used in the treatment of solar keratoses and BCC [18]. Imiquimod stimulates toll-like receptors to increase the production of endogenous cytokines, such as TNF-α, interferon gamma and several interleukins. It also has anti-angiogenesis activity [11]. As with other topical agents, the principal adverse effects are related to local site reactions – itch, redness, swelling and tenderness. More serious side effects include pigment changes, fever, diarrhoea, joint and muscle pain, psoriasis, vitiligo and angioedema [15, 18].


The inflammatory response caused by ingenol mebutate results in the release of cytokines and also antibodies directed against the tumour. It is used in the treatment of solar keratoses, and is under investigation for the treatment of BCC. Adverse effects associated with this treatment include redness, scaling and crusting of the skin in the area of application.
Radiotherapy


Radiotherapy is generally not used in younger patients because cosmetic results tend to wane over time. It cannot be performed in patients who have xeroderma pigmentosum or connective tissue disorders. Complications arising from radiotherapy are largely related to the dose administered. The higher the dose, the more likely complications are to develop. The side effects are also related to the site of treatment. Radiation therapy to the groin or armpit lymph nodes, for example, may result in swelling of the arms and legs due to poor fluid drainage.
Side effects of head and neck radiotherapy include [19]:
- Alopecia (hair loss)
- Desquamation
- Changes in pigmentation
- Parotiditis
- Mucositis
- Hearing loss
- Damage to the eyes
- Osteonecrosis
Surgery
Mohs surgery can be used for the management of SCC, BCC and melanoma. It is a surgical procedure that involves removing the lesion and some of the surrounding normal tissue. The specimen excised is then examined under the microscope to ensure that there are no tumour cells in the margin; if tumour cells are present, more tissue is excised and examined until there are no tumour cells visualised. This helps to ensure that there is good clearance whilst preserving as much normal tissue as possible [8].
More commonly, skin cancers are removed in a procedure known as an excision biopsy, where the lesion and some of the surrounding skin is removed and sent to a pathology laboratory for histopathological analysis. This method clears the lesion and the surrounding skin. The procedure is often performed in the doctor’s clinic under local anaesthesia. It is a cheaper, more practical alternative to Mohs surgery, however, it does not come with as much certainty that the excision margins are clear from tumour cells.
References
[1] Cancer Council Australia. 2014. Skin Cancer. http://www.cancer.org.au/about-cancer/types-of-cancer/skin-cancer.html
[2] Whiteman DC, Whiteman CA & Green AC. Childhood sun exposure as a risk factor for melanoma: a systematic review of epidemiologic studies. Cancer causes and control2001;12:69-82
[3] Stern RS, Weinstein MC, & Baker, SG. Risk reduction for nonmelanoma skin cancer with childhood sunscreen use. Arch Dermatol 1986; 122(5):537-545
[4] Usatine R.P., Smith M.A., Chumley H.S., Mayeaux E.J., Jr. (2013). Chapter 166. Actinic Keratosis and Bowen Disease. In Usatine R.P., Smith M.A., Chumley H.S., Mayeaux E.J., Jr. (Eds), The Color Atlas of Family Medicine, 2e.
[5] Duncan K.O., Geisse J.K., Leffell D.J. (2012). Chapter 113. Epithelial Precancerous Lesions. In Goldsmith L.A., Katz S.I., Gilchrest B.A., Paller A.S., Leffell D.J., Wolff K (Eds),Fitzpatrick’s Dermatology in General Medicine, 8e
[6] National Cancer Institute. Common moles, dysplastic nevi and risk of melanoma. 2011. http://www.cancer.gov/cancertopics/factsheet/Risk/moles
[7] Grossman D, David J. L (2012). Chapter 114. Squamous Cell Carcinoma. In Goldsmith L.A., Katz S.I., Gilchrest B.A., Paller A.S., Leffell D.J., Wolff K (Eds),Fitzpatrick’s Dermatology in General Medicine, 8e
[8] Belkin D., Carucci JA. Mohs surgery for squamous cell carcinoma. Dermatol Clin 2011;29(2):161-174
[9] Urba W.J., Washington C.V., Nadiminti H (2012). Chapter 87. Cancer of the Skin. In Longo D.L., Fauci A.S., Kasper D.L., Hauser S.L., Jameson J, Loscalzo J (Eds),Harrison’s Principles of Internal Medicine, 18e.
[10] Carucci J.A., Leffell D.J., Pettersen J.S. (2012). Chapter 115. Basal Cell Carcinoma. In Goldsmith L.A., Katz S.I., Gilchrest B.A., Paller A.S., Leffell D.J., Wolff K (Eds),Fitzpatrick’s Dermatology in General Medicine, 8e
[11] Hybarger C (2012). Chapter 9. Cutaneous Malignant Neoplasms. In Lalwani A.K. (Eds),CURRENT Diagnosis & Treatment in Otolaryngology—Head & Neck Surgery, 3e
[12] Bailey E.C., Sober A.J., Tsao H, Mihm M.C., Jr., Johnson T.M., Jr. (2012). Chapter 124. Cutaneous Melanoma. In Goldsmith L.A., Katz S.I., Gilchrest B.A., Paller A.S., Leffell D.J., Wolff K (Eds),Fitzpatrick’s Dermatology in General Medicine, 8e.
[13] Cole P, Heller L, Bullocks J, Hollier L.H., Stal S (2010). Chapter 16. The Skin and Subcutaneous Tissue. In Brunicardi F, Andersen D.K., Billiar T.R., Dunn D.L., Hunter J.G., Matthews J.B., Pollock R.E. (Eds),Schwartz’s Principles of Surgery, 9e.
[14] Lawley T.J., Swerlick R.A. (2012). Chapter 16. Atlas of Skin Manifestations of Internal Disease. In Longo D.L., Fauci A.S., Kasper D.L., Hauser S.L., Jameson J, Loscalzo J (Eds),Harrison’s Principles of Internal Medicine, 18e
[15] Galiczynski EM, Vidimos AT. Nonsurgical treatment of nonmelanoma skin cancer. Dermatol Clin, 2011;29(2):297-309
[16] Kuflik EG. Cryosurgery updated. J Am Acad Dermatol, 1994;31(6):925-44
[17] Kuflik EG. Cryosurgery for skin cancer: 30 year experience and cure rates. Dermatol Surg, 2004;30(2):297-300
[18] Micali G, Lacarrubba F, Nasca MR, Schwartz RA. Topical pharmacotherapy for skin cancer: Part I pharmacology. J Am Acad Dermatol, 2014;70(6):965.e1-12
[19] Hulyalkar R, Rakkhit T, Garcia-Zuazaga J. The role of radiation therapy in the management of skin cancer. Deramtol Clin, 2011;29(2):287-296.
Author: Ashleigh Elkins