


Psoriasis is a skin condition that affects about 2% of the population. Scaly, red patches develop and the skin may become itchy and flaky. It can affect nearly any site on the body, but is commonly found on the scalp, the elbows and on the knees. Other parts of the body that may be affected include the nails, palms of the hands and the soles of the feet.
Cause

Some genetic markers have been linked to psoriasis and may be important in the development of the disease, however, not all people with these markers develop psoriasis. One theory is that people who have inherited a genetic susceptibility to psoriasis have the condition triggered by an external factor. Some of the proposed external factors include stress, infection, smoking, medications, injury, alcohol and obesity.
People with HIV/AIDS, particularly in the later stages of the disease, can also develop psoriasis. Psoriasis tends to be more severe in HIV patients. It is not uncommon for sufferers of psoriasis to report a family history of the condition.
Psoriasis treatment
Several treatment options exist for psoriasis, however, there is no cure for the condition. The type and strength of treatment depends on the severity of the disease. Topical therapy, in the form of creams and ointments, is used for mild disease, whereas people with severe psoriasis may need to take tablets.
- Topical therapy: involves applying creams and ointments to the affected area of skin. Some of these are available over the counter without a prescription. The creams which tend to be most effective contain a corticosteroid. The steroid in the cream tones down the immune system and the inflammatory response occurring in the region where the psoriasis lesions are. It is wise to seek the advice of your doctor as to which the best cream is for the affected area. Other types of creams and ointments that are available include vitamin D (calcipotriol) creams, coal tar based creams and shampoos and vitamin A treatments (retinoids). These agents have varying effectiveness.
- Phototherapy: is often used for moderate cases of psoriasis and uses UV light to treat psoriasis.
- Systemic drug therapy: this form of treatment tends to be reserved for people with severe cases of psoriasis. Oral medications used for psoriasis include cyclosporine, methotrexate and acitretin. There is also range of drugs called biological agents. These medications target highly specific parts of the immune system involved in causing psoriasis. They are very expensive and will only be subsidised by the government if the patient has not responded to standard treatments. Regular check-ups are required whilst taking any of the above medications to monitor for side effects.
Lifestyle changes are also important to help control and manage your psoriasis. Smoking can make your psoriasis worse, so quitting (or the very least, cutting down) can help to control your symptoms. Keeping a healthy, well-balanced diet and regular exercise can also help. Moisturisers can also help to improve your psoriasis and make it more comfortable. Stress is also a key factor for some people with psoriasis, so learning to manage and reduce stress where possible can also make a difference.
Effects of psoriasis
Psoriasis can affect one’s self-esteem. The lesions themselves are uncomfortable for some and may be embarrassing. Wearing lighter coloured clothing, rather than dark colours can help reduce the visibility of the flakes on clothes. Women tend to be more affected by psoriasis psychologically than men.
Psoriasis can also affect physical health. A number of people with psoriasis also develop a type of arthritis, called psoriatic arthritis. There is also a higher risk of heart attacks and strokes in people with psoriasis.
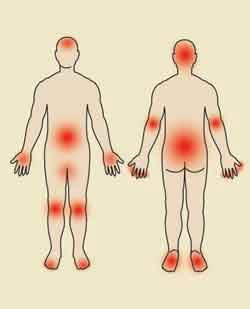
Psoriatic arthritis
Psoriasis sufferers may develop painful joints. The end joint in the fingers and toes (also known as the distal interphalangeal joint), the sacrum (in the lower back), ankles, knees and wrists tend to be affected most commonly. Affected joints are very painful and can be stiff and swollen. There may also be changes in fingernails and toenails.
There is no cure for psoriatic arthritis, but it can be managed with medications and keeping active and engaging in exercise. As with many types of arthritis, there may be flare-ups. People with psoriatic arthritis are often referred to a rheumatologist, who specialises in arthritis, to work out the best course of treatment. Some of the biological drugs discussed above may be given to control the joint symptoms as well as the skin manifestations. Other possible options include disease modifying anti-rheumatic drugs (or DMARDs), such as methotrexate, or non-steroidal anti-inflammatory drugs (such as nurofen, voltaren and celebrex).
Psoriasis can be difficult to effectively control. Dermatologists are highly experienced in managing this chronic condition. If you have any questions or concerns about your psoriasis, contact our clinic for an appointment. Contact us today.