


About excessive sweating
Hyperhidrosis is a condition characterised by excessive sweating. It is an embarrassing issue often affecting one’s self-esteem and self-confidence. There are various causes of hyperhidrosis, and thankfully, there are a number of treatments that are available.
Description
Hyperhidrosis is defined as the increased production of sweat disproportionate to the amount required to compensate for the body’s thermoregulatory needs and/or environmental conditions1. Hyperhidrosis is classified as primary or secondary and/or focal or generalised. Focal hyperhidrosis affects one or more areas of the body. The areas most commonly affected by focal hyperhidrosis are the palms of the hands, soles of the feet, the axillae (armpits) and the face2. Generalised hyperhidrosis affects the entire body and tends to be due to another underlying disorder3. Primary hyperhidrosis only occurs during waking hours, with sweating ceasing at night1. Primary hyperhidrosis tends to start in childhood and puberty and occurs in otherwise healthy individuals, whereas secondary hyperhidrosis is the result of another condition2.


Epidemiology
Hyperhidrosis affects 3% of the population. It afflicts equal numbers of men and women. Particularly with focal hyperhidrosis, family history is an important factor, with nearly 2/3 of patients with focal hyperhidrosis reporting a positive family history of the condition1. Hyperhidrosis is believed to be linked to chromosome 142. On average, the age of onset of hyperhidrosis is 25; however, palmar and axillary hyperhidrosis may have an earlier age of onset during adolescence. The majority of patients with hyperhidrosis are aged between 25 and 64 years3.

Aetiology
A number of underlying disorders can produce generalised hyperhidrosis. Some of the identified causes of generalised hyperhidrosis are listed below. Some of these disorders are very rare.
Causes of Generalised Hyperhidrosis1
1. Endocrine/Hormonal
- Menopause
- Hyperthyroidism
- Diabetes
- Hyperglycaemia
- Pheochromocytoma
- Hyperpituitarism
- Carcinoid syndrome

2. Medications

- Propranolol
- Tricyclic antidepressants
- Cholinesterase inhibitors
- Selective serotonin reuptake inhibitors
- Opioids
3. Infections
- Endocarditis
- Malaria
- Tuberculosis
- HIV
4. Neurological
- Parkinson’s disease
- Brain lesions
- Peripheral neuropathy (eg. diabetic, alcoholic)


5. Congestive Cardiac Failure
6. Cancers
The most common cause of focal hyperhidrosis is primary idiopathic hyperhidrosis. Primary hyperhidrosis is due to over-activity of the sudomotor sweat control system, without a recognised trigger4. This condition is poorly understood. In order to make a diagnosis of primary focal idiopathic hyperhidrosis, a number of diagnostic criteria need to be met. The diagnostic criteria states that a patient needs to have a 6 month history of focal, visible and excessive sweating with no other apparent cause, and have at least two of the following:
- Bilateral, relatively symmetrical pattern of sweating
- At least one episode of excessive sweating per week
- Profound impact on daily activities
- Onset at age 25 or less
- Family history of hyperhidrosis
- Sweating which ceases at night1,2,3
Other causes of focal hyperhidrosis include neurological causes, including neuropathy and spinal cord injury, and Frey’s syndrome3. Frey’s syndrome is a recognised complication of parotidectomy; a surgical procedure to remove the parotid gland; a large salivary gland which is located in front of the ear. One of the nerves innervating the parotid gland can be damaged during this procedure. The damaged nerve forms a network with other nerves innervating the sweat glands of the face. When presented with food, or other gustatory stimuli, the sweat glands are activated causing flushing of the face and excessive sweating2. Focal hyperhidrosis can also occur secondarily to generalised anxiety disorder; this is because the eccrine sweat glands can be activated in response to emotional stimuli5.
Diagnosis
Diagnosis of hyperhidrosis is often made based on the presenting signs and symptoms, a careful medical history and physical examination. The severity of the condition is assessed using a subjective tool, known as the hyperhidrosis disease severity scale. This is a 4 point scale classifying different severities of the disease:
- My sweating is never noticeable and never interferes with my daily activities
- My sweating is tolerable but sometimes interferes with my daily activities
- My sweating is barely tolerable and frequently interferes with my daily activities
- My sweating is intolerable and always interferes with my daily activities4.
The higher the score on this scale, the greater the severity of the disorder and the greater the impact of the disease on the patient’s quality of life4.
Sometimes patients have an iodine starch test. In this test, iodine is applied to dry skin and then starch is sprinkled on top. Sweat reacts with the iodine and starch and causes the skin to turn a dark colour1. This is commonly used prior to injection for sweating treatment to help map the area of skin that needs to be treated, as well as prior to iontophoresis to determine the efficacy of the treatment.
Pathophysiology
The pathophysiology underlying hyperhidrosis is poorly understood. The autonomic nervous system is thought to be largely implicated in the underlying pathophysiology of the disease, with input from emotional stimuli and genetics4. The sweat glands of the body are innervated by nerves of the autonomic nervous system, specifically the sympathetic division, which is involved in the ‘fight or flight’ response. An important anatomical structure in the sympathetic nervous system is the sympathetic chain. The sympathetic chain consists of nerve fibres and ganglia (collections of nerve cell bodies), and runs from the base of the skull to the coccyx. The nerve supply to the axillary and palmar sweat glands is derived from the thoracic and lumbar portions of the sympathetic chain2. This has an implication for the surgical treatment of this condition, which is discussed later.
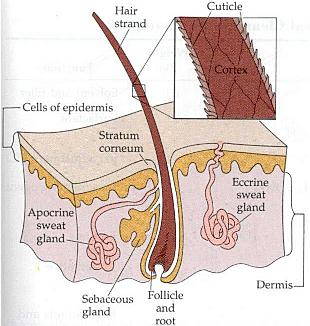

Three types of sweat glands have been identified in the human body – eccrine sweat glands, apocrine glands and apoeccrine glands. The different types of sweat glands are described below (adapted from[6]):
1. Eccrine
- Location: Distributed throughout the skin of the entire body, high concentration in the palms and the soles
- Structure: Secretory portion is coil-shaped and has a narrow lumen. The duct is long, thin and opens onto the surface of the skin
- Innervation: Sympathetic nerve fibres; Neurotransmitter acetylcholine
- Development: Present at birth
- Association with hair follicle: No association with hair follicle
- Function: Regulation of body temperature (thermoregulation)
2. Apocrine
- Location: Axillae, anus, genital region, umbilicus, nipples
- Structure: The secretory portion is coil-shaped, but has a wide lumen. The duct is short and thick and opens into the hair follicle
- Innervation: Unknown, believed to be humoral involving β-agonists
- Development: Present at birth
- Association with hair follicle: Associated with the terminal part of hair follicles
- Function: Unknown, possible role in the communication of smells
3. Apoeccrine
- Location: Axillae
- Structure: The secretory coil portion has a combination of apocrine and eccrine features; the duct is long and opens onto the skin, taking on a more eccrine morphology
- Innervation: Sympathetic nerve fibres; Neurotransmitter Acetylcholine
- Development: Not present prior to adolescence
- Association with hair follicle: No association with hair follicles
- Function: Unknown, possible thermoregulatory role
Eccrine and apoeccrine glands are the sweat glands involved in hyperhidrosis; apocrine glands play no role in the pathology of this disorder6. Despite the involvement of eccrine and apoeccrine glands in the pathology of hyperhidrosis, there is no increase in the numbers of these glands, nor are there any structural or histological changes to the glands. There are also no histological changes to the sympathetic nerves innervating the glands; hence, the underlying pathology is thought to be due to either over-activity or hyper-excitability of the sympathetic nerves and autonomic nervous system innervating the glands and/or an abnormal increase in baseline sweat secretion due to emotional or environmental stimuli2.
Treatment
Several treatment options are available for sufferers of hyperhidrosis. Non-surgical and surgical options are available. Despite the numerous treatment options which are available, only 1/3 of patients seek treatment from their general practitioner. Treatment is important; hyperhidrosis causes not only physical discomfort, but a number of psychosocial issues. It affects the individual’s day to day functioning, confidence and performance at work. Sufferers of hyperhidrosis also have higher rates of depression1.
Non-Surgical Management
Aluminium Chloride Deodorants
Aluminium chloride is a compound that is found in many anti-perspirant deodorants available at supermarkets, but it is in a low concentration. Aluminium chloride is used as the first line of treatment for mild to moderate hyperhidrosis, especially of the axilla2. Aluminium chloride works by blocking the duct of the eccrine sweat gland, preventing the release of sweat onto the skin. The aluminium chloride salts form complexes with compounds in the skin known as mucopolysaccharides; this complex then move into and block the eccrine sweat gland ducts in the lower to mid epidermis2,4. It is recommended that a preparation containing 10-15% of aluminium chloride should be applied to the affected area or areas of skin at night just prior to going to bed when the skin is dry, generally every 24 to 48 hours for 3 to seven treatments at first. After two weeks, the regimen can be reduced to a once-weekly application2,4. If there is no response to this treatment, the strength of the preparation can be increased to 25 or 35%; it is also important to ensure that the solution has been in contact with the skin for at least 6-8 hours prior to being washed off2.

Aluminium chloride has a success rate of up to 90%, has very few side effects, and those that do occur are largely reversible. The main disadvantage of aluminium chloride anti-perspirants is that they last for a short duration in comparison to other treatments. Local reactions have also been reported, including a burning sensation and irritation in the local area of skin that the treatment has been applied to4. If these skin irritations do occur, the anti-perspirant can be combined with a 1% solution of hydrocortisone to limit the irritation1. Aluminium chloride anti-perspirants are available for purchase at pharmacies.
Oral Medications
Anticholinergic drugs are used in the treatment of hyperhidrosis which is refractory to topical treatments. Glycopyrrolate is one agent that is commonly used. It works by inhibiting the cholinergic muscarinic receptors, which blocks the transmission from the sympathetic nerve fibres to the eccrine sweat glands, resulting in decreased sweating. However, the drug also affects other systems which rely on cholinergic transmission, resulting in side effects such as urinary retention, fast heart rate (tachycardia), dry mouth, blurry vision and orthostatic hypotension (a drop in blood pressure when standing up after sitting or lying down)2.

Antidepressant drugs have also been used in the treatment of hyperhidrosis, especially in patients who suffer from co-morbid depression and/or anxiety disorders. Paroxetine and fluoxetine have been shown to produce mild improvements in both hyperhidrosis and anxiety7. Paroxetine and fluoxetine are both selective serotonin reuptake inhibitors and are believed to act centrally, modulating the emotional input which is involved in the disorder. Quetiapine has also been reported as a treatment for hyperhidrosis. This agent has few side effects and is believed to have a central action modulating emotional input of the disorder, as well as decreasing the excitation of sympathetic neurons. However, this is not a widely used treatment and is largely experimental7.
Iontophoresis
Iontophoresis is another non-surgical treatment that is beneficial for the treatment of palmar and plantar hyperhidrosis. Iontophoresis is defined as the introduction of an ionised substance through the intact skin by applying a direct current8. Moisturised pedals are applied to the skin. The pedals are also in direct contact with a solution containing electrolytes. A current is passed through the electrolyte solution. The treatment aims to cause reversible disruption of the ion channels4. The exact mechanism of action of iontophoresis treatment is unclear. Changes in the structure of the sweat glands have not been observed; nor has blockage of the sweat gland ducts. It is thought that iontophoresis alters the resorption of sodium ions in the sweat glands, as the sodium concentration and volume of sweat produced decreases following this treatment8. Typically, tap water is used in the solution. However, the addition of anticholinergic drugs to the tap water can improve the efficacy of iontophoresis, as well as increase the duration of the effects of the treatment4.


Iontophoresis is used as a first line treatment for moderate to severe hyperhidrosis of the palms of the hands and soles of the feet. It is difficult to treat facial and axillary hyperhidrosis by this method2. The efficacy of iontophoresis is high, with a reported success rate of 81%. Iontophoresis is not suitable for use in pregnant women, and also cannot be used in patients with pacemakers. Side effects are temporary and include transient irritation of the skin, pain and blistering; with no reported long term adverse effects4. But, the treatment is time consuming and some patients do not find it pleasant. The machines are also expensive, and maintenance treatment is also required4.
Injections for sweating
Injections may be used in the treatment of hyperhidrosis. The injection contains a neurotoxin which is produced by the bacterium clostridium botulinum. It works by causing irreversible inhibition of the release of acetylcholine from the pre-synaptic nerve terminal at the neuromuscular junction and the eccrine sweat glands8. Injections for sweating are primarily used in the treatment of axillary hyperhidrosis. The injections can reduce the amount of axillary sweating by around 85 % 8.
The area of the axilla involved in the excessive sweat production is treated. Multiple injections are delivered at a distance of 1-2cm apart. The effects of injections for sweating only last for a certain period of time and the injections may need to be repeated; the effects of treatment tend to last between 4-18 months. The maximum dose of the injection that can be administered in one treatment is 100U. Local anaesthesia can be used to minimise the discomfort associated with the injections4.
These injections cannot be used during pregnancy and the treatment is contraindicated in patients with diseases of the neuromuscular junction, such as myasthenia gravis, as well as patients with blood coagulation disorders. The main drawbacks of injections for sweating treatment are that the effects are not permanent and the need to repeat the treatment4.
Adverse effects associated with injections for hyperhidrosis are uncommon. The main reported adverse effects include mild pain at the injection sites and compensatory hyperhidrosis in untreated areas. The latter complication tends to be mild and has only been reported in about 5% of patients8. The treatment works quickly, with patients noticing a reduction in sweating between 2 and 4 days after the injection. The greatest effects are observed at 2 weeks after the treatment8.
Surgical Management
If the aforementioned non-surgical treatment measures of hyperhidrosis treatment are unsuccessful, surgical treatments can be considered.
Retrodermal Curettage/Liposuction
Retrodermal curettage is a minimally invasive surgical procedure. The curette is used to remove the sweat glands underlying the skin. This procedure is generally performed in the axilla. After removal of the sweat glands, the area is washed out and a drain is inserted. The wound is then sutured. The procedure can be performed under local anaesthesia4. Retrodermal liposuction is a similar procedure which uses a liposuction cannula through a small incision to remove the sweat glands in the axilla. Both methods improve axillary hyperhidrosis significantly; and the effects are permanent in most people; with recurrence rates of 7-8%. Side effects are both immediate and long term. Immediate side effects tend to be post-operative complications, such as bleeding, infections and pain. Long-term side effects include scarring, alopecia (hair loss), changes in the colour of the skin and impairments in the range of motion of the arm4.


Thoracoscopic Sympathectomy
Sympathectomy is a surgical procedure which involves removal of one or more sympathetic ganglia in the sympathetic chain. The aim of the procedure is to stop the sympathetic supply to the affected area and hence remove the innervation to the sweat glands. Depending on the area to be treated, different levels of the sympathetic trunk are removed. Below lists the levels of the sympathetic trunk and the regions that they supply (Adapted from [8]):
- T1: Head
- T2: Neck
- T3-6: Thorax
- T7-11: Abdomen
- T12-L2: Legs
- T2-3: Hands
There are certain patient characteristics that should be considered in determining whether one is suitable to undergo thoracoscopic sympathectomy. Those who are deemed to be good candidates for the procedure are those who experienced disease onset at an early age (during adolescence), are young (<25) at the time of the procedure, do not sweat at night, have a body mass index below 28 and are in good general health9. Thoracoscopic sympathectomy produces better results for palmar hyperhidrosis than it does for axillary hyperhidrosis9. Overall, patients are satisfied with the outcome of the procedure, with patient satisfaction rates reported as high as 85%8.
There are a number of complications associated with performing thoracoscopic sympathectomy; these should be considered and discussed thoroughly as the entire point of the procedure is to improve quality of life for sufferers. Compensatory hyperhidrosis is one of the most common side effects of the procedure; however, there are highly variable rates of this complication reported in the literature – ranging from 3% to 98%9. Other more common complications include Horner’s syndrome, pneumothorax and bradycardia (slow heart rate). Rare complications of the procedure are haemothorax, pleural effusion, chylothorax and persistent intercostal neuralgia9.
References
[1] Perera E, Sinclair R. Hyperhidrosis and bromhidrosis: A guide to assessment and management. Australian Family Physician, 2013;42(5):266-269
[2] Smith FCT. Hyperhidrosis. Surgery, 2013;31(5):251-255
[3] Haider A, Solish N. Focal hyperhidrosis: diagnosis and management. CMAJ, 2005;172(1):69-75
[4] Vorkamp T, Foo FJ, Khan S, Schmitto JD, Wilson P. Hyperhidrosis: Evolving concepts and a comprehensive review. The Surgeon, 2010;8:287-292
[5] Woolcock K. Smelly Feet. Australian Pharmacist, 2011; 30(7):564-568
[6]Schaller M, Plewig G. Chapter 35: Structure and function of eccrine, apocrine and sebaceous glands. In Bolognia JL, Jorizzo JL, Schaffer JV. 2012. Dermatology, 3rd edition. Saunders-Elsevier
[7] Dickmann LM, Dickmann JRM. Quetiapine in the treatment of hyperhidrosis axillaris. British Journal of Dermatology, 2010;163(5):1126-1127
[8] Walling HW, Swick BL. Treatment options for hyperhidrosis. Am J Clin Dermatol, 2011; 12(5):285-295
[9] Cerfolio RJ, de Campos JRM, Bryant AS, Connery CP, Miller DL, et al. The society of thoracic surgeons expert consensus for the surgical treatment of hyperhidrosis. Ann Thorac Surg, 2011; 91:1642-1648
Author: Ashleigh Elkins