


When hair loss or severe hair thinning occurs, it can be called balding, hair loss, or alopecia. The term Androgenic Alopecia is an inherited condition that relates directly to hormonal hair loss. It is extremely prevalent within the general population. Androgenetic alopecia is broken down into male and female patterned hair loss.
The distinctions between the two are quite simple:
- Male pattern baldness – this is the type of hair loss that is defined as the ‘receding hair line’ version, and also by the ‘monk’s’ pattern of hair loss at the top of the head and spreading outward; and
- Female pattern baldness – this is the type of hair loss that is defined by the thinning of hair at the very top of the scalp (known as the vertex), and it is usually much less severe than that of male baldness
This type of alopecia is different than alopecia areata because it has a recognisable pattern instead of a random scattering of patches of hair loss. Additionally, the androgenic variants may be much slower in their progression than other types of alopecia.
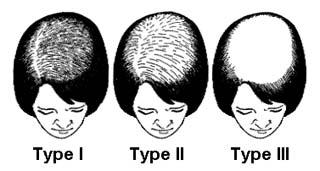
Male Pattern of Hair Loss
Males and females experience loss of hair in different areas of the scalp. Males tend to lose hair in the following sites:
- The temporal area, known as a receding hairline
- Over the frontal part of the scalp
- In the vertex (top, back) of the scalp
Female Pattern of Hair Loss
Women are affected differently to men by androgenetic alopecia. The frontal part of the scalp (fringe area) is rarely affected in women. Women tend to experience thinning over the crown of the head. Although women may experience loss in the temporal region (receding hairline), this is an unusual presentation in a female. The loss of hair in women is typically less severe than what is observed in males.
The Hair Cycle
Hair grows in three main stages; the anagen phase, the catagen phase and the telogen phase. The three stages all occur concurrently over the scalp of a human. At the same time, some hairs are in the telogen phase, whilst others are in the anagen or catagen phase. About 85% of hairs are in the anagen phase, which is the active phase of growth. This phase can last up to 6 years; with the length of the anagen phase being determined by individual genetics. The catagen phase is a transition phase in which the follicle renews itself and the hair is detached from its blood supply. The catagen phase lasts approximately 2 weeks. The third stage is the telogen phase; this is a resting phase where the follicle is not active. About 15% of the hairs on the head are in the telogen phase at any given point. The hair is still there, but it is not receiving any nourishment and is in a resting state. Eventually, the follicle becomes active and grows again, pushing the hair off, resulting in hair shedding, and the anagen phase begins again.
What Happens in Androgenic Alopecia
Androgenetic alopecia is an inherited disorder that is the result of a heightened sensitivity to one of the male hormones (androgens), dihydrotestosterone. Only certain areas of the scalp are more sensitive to the effects of the hormone and these are the areas affected by the loss of hair. Despite being thought of as a ‘male’ hormone, dihydrotestosterone is still present in females, albeit at much lower levels. Females who are affected may have an androgen excess disorder, such as polycystic ovarian syndrome (PCOS), in addition to the genetic predisposition. Dihydrotestosterone is found in many sites across the body, of which one is the scalp. Dihydrotestosterone is responsible for reducing the length of the anagen phase from its normal duration of up to 6 years, to as short as a few weeks. As a result, the hair follicles shrink and produce fewer hairs. Treatments are targeted at dihydrotestosterone.
Associated Conditions
In women, the main associated condition with androgenetic alopecia is PCOS. PCOS is associated with weight gain, an increased risk of developing diabetes, excess hair, irregular menstrual cycles, fertility issues and acne. In males, androgenetic alopecia is linked with prostate hyperplasia and prostate cancer, coronary heart disease, high blood pressure, insulin resistance and diabetes. Additionally, some women can present with male pattern hair loss. These women tend to suffer from androgen excess disorders, such as congenital adrenal hyperplasia. A minority of women suffering from PCOS experience a male pattern of hair loss.
Genetics
The AR gene has been implicated in the genetics of androgenetic alopecia. The AR gene codes for the androgen receptors found on the surfaces of cells and tissues which are responsive to androgens; including the hair follicles. Slight mutations and variations to this gene can alter the expression of the gene (ie. the number and sensitivity of the androgen receptors in the tissues and hair follicles), predisposing people with the variant gene to androgenetic alopecia. The AR gene is so far the only gene that has been identified and implicated in androgenetic alopecia, but it is widely believed that there are other genes that play a role in the development of the condition.
Treatment
The treatments vary according to the severity of the condition and the desire of the patient to pursue a remedy. Treatment may be important for some people as androgenetic alopecia can affect self-esteem and lead to mental health issues, including depression.
A number of different medications are used in the treatment of androgenetic alopecia. Minoxidil may be used as either a topical or oral preparation. It is more effective in patients in the early stages of the condition and more effective at higher strengths. The precise mechanism by which minoxidil works is not known, but it increases the amount of time the hairs spend in the anagen phase. It is also thought to improve the blood supply to the hair follicles. Importantly, treatment with minoxidil needs to be continued indefinitely. If treatment is ceased, the hair returns quickly to its pre-treatment state.
Another medication that is used in the treatment of androgenetic alopecia is finasteride. The medication has not been proven to be effective in post-menopausal women. It is taken orally. It is most effective against hair loss on the vertex of the head. Not only does it slow progression of androgenetic alopecia, but it also can stimulate new growth in affected areas. As with minoxidil, the medication should not be ceased. If stopped, the hair loss will only progress. Finasteride works by inhibiting the 5-alpha reductase enzyme. This enzyme acts on testosterone to convert it to dihydrotestosterone.
In females, anti-androgen medications such as spironolactone and cyproterone acetate may be prescribed in suitable patients.
Topical formulations of the above medications can be used for androgenetic alopecia. Most of these have not been studied in proper double-blinded and randomised clinical trials. They may help to prevent progression of hair loss in some people. Added hair growth is usually a bonus. They may be trialled in patients unwilling or unable to take oral medications.
Other potential treatment options include hairpieces, toupees, hair transplantations and tattooing.
If you have any questions or concerns about androgenetic alopecia and its treatments, you are welcome to contact us today.